


The Evolution of CDC Vaccine Recommendations
Aging boomers may not be the main reason the US health care industry is growing...


Here is what I compiled based on the CDC vaccine schedule history for the following groups: 0-2 years, 2-18 years, 19-70 (healthy), and 19-70 (high risk). A few takeaways:
The vaccine schedule from birth to 24 months gradually expanded from 5 total injections to 26 total injections following passage of the National Childhood Vaccine Injury Act of 1986 (Graph 1).
The spike in total injections for children 2-18 years old after the year 2000 is attributable to the introduction of annual flu shots taken over a 16-year time span (Graph 2).
"High risk" adults always received more vaccines, but in 2013 the number of vaccines given to healthy adults “caught up” with the number previously reserved for high risk adults. Shortly thereafter, the CDC came up with even more shots to reserve for high risk adults (Graph 3.1).
Originally flu shots were limited to elderly and other high risk adults, then in 2012 these annual shots were recommended to all groups of adults (Graph 3.2).
Table 1:
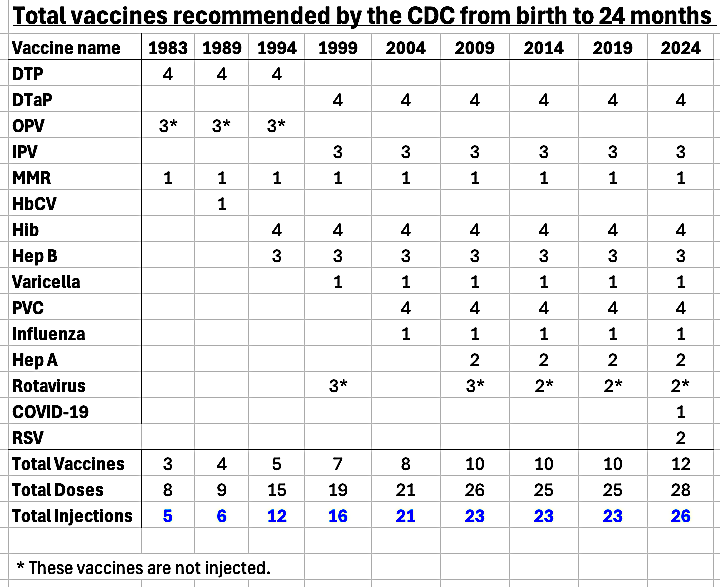
Graph 1:

Table 2:

Graph 2:

Table 3A:
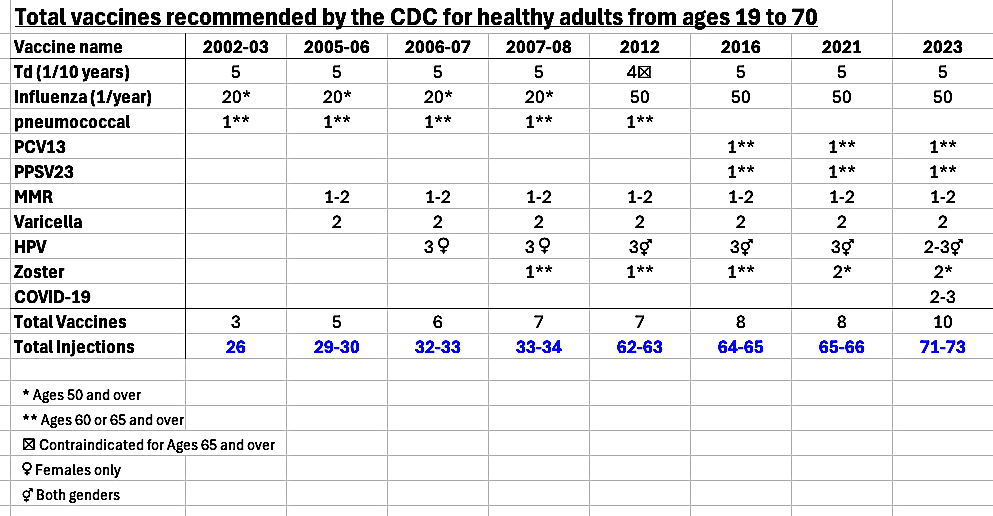
Table 3B

Graph 3.1:

Graph 3.2

Some months ago I cited an article from Our World in Data highlighting how data points representing both US health care costs AND life expectancy started to deviate from those of their OECD counterparts in 1985 (Graph 4). This trend started long before the start of the opioid crisis (circa 2005-2010) and somewhat coincided with expansion of the childhood vaccine schedule.
If these injections are doing more harm than good, then the quadrupling of shots given to US toddlers between 1990 and 2005 (Graph 1) could have played a key role in exacerbating the trend had started in 1985, and the subsequent expansion of annual flu shots to adults of all ages only further escalated the insult to injury that previously targeted toddlers and “high risk” adults (Graphs 2 and 3.1).
Graph 4: M. Roser (2020) Why is life expectancy in the US lower than in other rich countries? Our World in Data.

In 1913, Charles Richet was awarded a Nobel Prize for his pioneering work on “anaphylaxis,” whereby test animals were sensitized to minimally toxic substances via injection. Near the end of his acceptance speech, the French physician concluded:
We are so constituted that we can never receive other proteins into the blood than those that have been modified by digestive juices. Every time alien protein penetrates by effraction, the organism suffers and becomes resistant. This resistance lies in increased sensitivity, a sort of revolt against the second parenteral injection which would be fatal.
In effect, Richet was discussing the shortcomings of intramuscular injection AND central role of membrane barriers in processing substances entering the body …over a century ago!
To my knowledge, the only research to date addressing the concern of anaphylaxis via injected vaccines is a Japanese study that linked a gelatin allergy epidemic to newly-formulated gelatin-containing DTaP injections given to Japanese babies in the 1980’s (Table 4). While I am grateful to Sakaguchi and Inouye for this valuable contribution I am disgusted that nothing like this has been published in the US.
Table 4: Masahiro Sakaguchi and Sakae Inouye (2000) “Systemic Allergic Reactions to Gelatin Included in Vaccines as a Stabilizer.” Japanese Journal of Infectious Disease 53: 189-195.

In 1847 Ignaz Semmelweis demonstrated the critical role of hand-washing in maternity clinics. This discovery was so unsettling that a maternity institute professor in Germany committed suicide after realizing he might have transmitted the infection that killed his cousin. Semmelweis for his part never lived to see his ideas widely accepted: He was beaten to death within a few days of being committed to an insane asylum in 1865.
I shudder to think how modern-day pediatricians trained to browbeat parents into submission come to terms with the truth over their role in this silent atrocity. Far better to speak out and die a “madman” than to drown in a sea of remorse after running out of time to make amends…
This link is where I got my information. Even though I tried my best in summarizing what I understood I welcome corrections to this work in progress...
The kid gets the quackzine fever then gets the NSAID then - WOOSH - mush brain. Like a binary weapon.
Everybody knows that the kid is out of the womb only because the pelvis is too narrow; the baby brain is still undergoing embryogenesis until puberty. So this idea to inject heavy metals while artificially inducing a fever & throwing in a potentially organ-devouring prostaglandin inhibitor is totally crazy - if not criminally insane - take your pick.